
The NeuRX Diaphragm Pacing System. The NeuRX DPS phrenic pacer, developed by Case Western’s; Ray Onders MD, FACP, may condition the diaphragm muscles in people with ALS by stimulating the phrenic nerve that controls these muscles through implanted electrodes. Recently approved by the FDA, the device is available by prescription to people with ALS that are battling chronic hypoventilation. Image: Synapse Biomedical.
Over 75% of people with ALS ultimately lose the battle with the disease due to respiratory failure. To combat the decline of the diaphragm muscles, physicians at Case Western Reserve University School of Medicine introduced a phrenic pacer called the NeuRX DPS in hopes to strengthen these muscles to bolster diaphragm function. Recently approved by the FDA, this device according to anecdotal evidence may delay the need for mechanical ventilation.
But some ALS experts argue that the NeuRX DPS has not yet been sufficiently demonstrated through clinical studies to slow respiratory decline or even improve the quality of the life of people with ALS. And with a cost of upwards of $20,000 USD, insurance providers may therefore be reluctant to cover this device for patients.
Now, University of Paris’ Groupe Hospitalier Pitié-Salpêtrière physicians in a preliminary study report that the NeuRX DPS may increase the stamina of the diaphragm muscles, helping people with ALS sleep more soundly.
The team found that patients implanted with the device after four months of diaphragm conditioning experienced a median increase in sleep efficiency of 9%, dropping the time awake after falling asleep by 40%, about one hour. 18 patients participated.
“Even if we would have shown a maintenance in sleep quality would have been a surprise,” says Thomas Similowski, Groupe Hospitalier Pitié-Salpêtrière Chief of Respiratory and Intensive Care Medicine who led the study. “Showing that we actually improve sleep efficiency is very spectacular.”
A larger study is now ongoing.
Keeping Pace
Phrenic pacemakers substitute for brain centers that become decoupled due to injury or disease from the neuronal circuitry controlling respiratory muscles by electrically signaling at regular intervals the diaphragm to contract, allowing patients to breathe without mechanical ventilation.
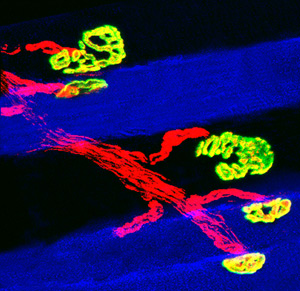
Just breathe. Phrenic nerve (red) impulses trigger the contraction of the muscles (blue) in the diaphragm, enabling us to breathe air in. Here, only slow muscle fibers and their attachments to nerve terminals called neuromuscular junctions (yellow) are shown. Image: Gary Sieck PhD, Mayo Clinic. Copyrighted and used with permission from the Mayo Foundation for Medical Education and Research. All rights reserved.
Harvard cardiologist Stanley Sarnoff MD first introduced the idea of phrenic pacing in 1944 to support breathing of a 5 year old boy who suffered from paralysis of the diaphragm. And in 1968, Yale cardiologists William Glenn MD and John Judson MD demonstrated that these devices can help regulate the breathing of a patient suffering from chronic hypoventilation – the inability to bring enough air into the lungs to support respiration. Introduced into routine clinical practice in the early 1970s, phrenic pacemakers are typically prescribed to support ventilation of people who suffer from spinal cord injuries or experience certain chronic sleep or breathing difficulties.
But physicians remained skeptical about whether or not phrenic pacemakers could benefit people with ALS. This is because the phrenic nerves in patients are deteriorating making it more difficult for these electrical impulses to reach the diaphragm. And at the same time, these nerves are inflamed and may be inadequately myelinated in places in people with ALS resulting in the inefficient delivery of these impulses, making it harder to stimulate the contraction of these respiratory muscles.
Physicians at Case Western Reserve University School of Medicine nevertheless suspected that phrenic pacemakers may help people with ALS. Their idea: these devices could strengthen the muscles in the diaphragm and thereby slow respiratory decline.
“They are applying stimulation not to produce ventilation,” explains Similowski, “but to train the diaphragm muscles.”
In 2007, a multinational team led by Case Western surgeon Ray Onders MD, FACP, launched a clinical trial in the United States and France to evaluate the potential benefits of the NeuRX DPS phrenic pacemaker in people with ALS with chronic hypoventilation. 86 patients participated.
The physicians found according to results submitted to the FDA that the device extended the median survival of participants 16 months than those in a comparable study supported by noninvasive ventilation alone. But the team was unable to definitively demonstrate that this device slowed respiratory decline in people with ALS – at least as determined by monitoring participants’ forced vital capacities.
”It looks like it may be helpful but the scientific evidence is truly lacking,” says Methodist Neurological Institute neurologist Stan Appel MD. “We just don’t know.”
Goodnight DPS
Take a deep breath. Breathing is powered by a choreographed dance of respiratory muscles featuring the diaphragm and intercostal muscles. Video: Tutor Vista.
But breathing is powered by much more than a diaphragm during waking hours. And forced vital capacity therefore evaluates the health of other respiratory muscles in the chest that are also deteriorating in people with ALS.
Groupe Hospitalier Pitié-Salpêtrière physicians decided therefore to take a look at people with ALS after bedtime. This is because the diaphragm alone powers breathing during sleep. By evaluating sleep quality of patients, the physicians could compare the function of the diaphragm before and after being conditioned.
“A decrease in breathing during sleep is a very sensitive marker of diaphragm dysfunction in ALS,” says Similowski. “That’s a very early marker of the disease.”
The team found that people with ALS stayed asleep longer and slept more soundly. But surprisingly, the team found that key indicators of diaphragm strength continued to decline such as Sniff Nasal Inspiratory Pressure (SNIP) – about 8% on average during the duration of the study.
The team speculates that this is because the device does not make the diaphragm stronger but instead boosts the stamina of these muscles by promoting the conversion of the fibers to so-called slow twitch ones that are designed for endurance. Typical tests such as those the team used according to Similowski predominately evaluate fast twitch fibers in the diaphragm which are designed for speed. Studies to test this idea are ongoing.
Before NIV?
Physicians at the University of Paris however suspect that phrenic pacemakers such as the NeuRX DPS can make more of difference for people with ALS. Anecdotal evidence suggests that the device may prolong the need for a mechanical ventilator up to 24 months. And suspects Similowski, conditioning the diaphragm just as these respiratory muscles start to deteriorate might even delay the time when noninvasive ventilation is needed.
Starting in 2012, Similowski’s team is launching a clinical trial to test just that. People with ALS experiencing the first signs of respiratory dysfunction with or without the NeuRX DPS implanted will be monitored for two years and compared. About 75 patients are expected to be enrolled. Results are expected in early 2015.
References
Gonzalez-Bermejo, J., et al. (2011) Diaphragm pacing improves sleep in patients with amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis. doi:10.3109/17482968.2011. 597862 Abstract | Full Text (Subscription Required)
Onders, R.P., et al. (2009) Complete worldwide operative experience in laparoscopic diaphragm pacing: results and differences in spinal cord injured patients and amyotrophic lateral sclerosis patients. Surgical Endoscopy, 23(7): 1433-1440. Abstract | Full Text (Subscription Required)
Sarnoff, S.J., Hardenbergh, E., and Whittenberger, J.L. (1948) Electrophrenic respiration. Science, 108(2089), 482. Full Text (Subscription Required)
Judson, J.P. and Glenn, W.W. (1968) Radio-frequency electrophrenic respiration. Long-term application to a patient with primary hypoventilation. Journal of the American Medical Association, 203(12), 1033-1037. Abstract | Full Text (Subscription Required)
Further Reading
Marion, D.W. (2011) Diaphragm Pacing. UpToDate. Excerpt | Full Text (Subscription Required)