Clinicians first turned to stem cells in the 1960s to treat severe combined immunodeficiency syndrome (SCID) – rearming the immune system to help fight off infections. The transplantation strategy, which involves repopulating the bone marrow with healthy adult stem cells, is now routinely used to treat blood cancers including leukemia and certain lymphomas and myelomas.
In the 1970s, researchers led by Harvard’s Howard Green MD learned to grow adult stem cells in the laboratory – regenerating patches of human skin. The stem-cell based strategy is the mainstay of treating severe burns in emergency rooms.
“Skin grafts [represent] 30 years of success of stem cells in a clinical setting,” says Rockefeller University’s Elaine Fuchs PhD.
A growing group of researchers, however, suspect that stem cells could hold the key to the treatment of a much larger number of conditions. Reprogrammed islet-stuffed “tea bags” developed by Harvard University’s Doug Melton PhD might soon deliver life-sustaining insulin to diabetics. Growth factor-soaked motor cortex patches pioneered by University of Toronto’s Molly Shoichet PhD may help the brain rebuild after a stroke. And, cellular models of disease may enable the discovery of more effective treatments for a wide range of neurological conditions including ALS.
In June, experts gathered at the 2013 meeting of the International Society of Stem Cell Research (ISSCR) in Boston to discuss the latest stem cell advances and the challenges of introducing stem cell-based therapies into the clinic going forward.
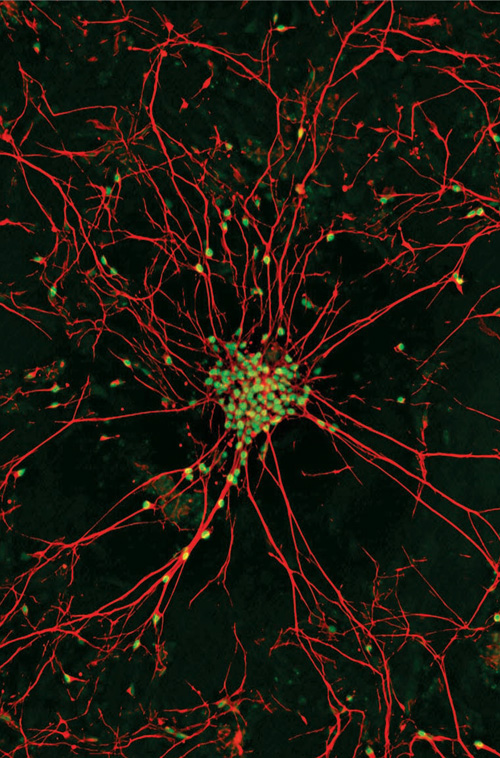
Modeling ALS Scientists are recreating motor neurons from people with ALS from skin biopsies in hopes to identify more effective treatments for the disease. Image: Gist Croft PhD and Mackensie Amoroso, then at Columbia University.
Stem cells – the next top model?
A new stem cell model may make identifying ALS medicines even easier according to studies led by University of Wisconsin’s Su-Chun Zhang PhD. Reprogrammed mutant superoxide dismutase 1 (SOD1) motor neurons appear to accumulate neurofilament aggregates – a major hallmark of the disease.
The buildup of neurofilaments may be a key contributor of ALS. Lowering levels of these aggregates according to early preclinical studies led by University of California San Diego’s Don Cleveland PhD delays onset and progression of a SOD1 mouse model of the disease.
The results suggest that potential medicines for ALS could be identified by screening for drugs that reduce the number of neurofilament aggregates.
The emerging stem cell model is one of a growing number of systems that are also being developed across the globe to discover underlying mechanisms of the disease.
Meanwhile, Harvard University Stem Cell Institute’s Kevin Kim PhD is gearing up to use similar systems to screen for potential therapies for ALS. The initiative, led by Harvard Stem Cell Institute’s Kevin Eggan PhD and Lee Rubin PhD, aims to identify medicines by screening for drugs that protect motor neurons from degeneration.
The screening approach uses a bank of stem cell lines obtained by reprogramming skin cells donated by people with multiples forms of ALS including SOD1 and TDP43-linked disease.
Drugs including riluzole appear to protect motor neurons derived from some people with ALS according to pilot studies presented at ISSCR 2013. But others including olesoxime, which recently failed in the clinic, appear to be ineffective.
The preliminary results suggest that such an approach might enable clinicians to create personalized treatment strategies for people with the disease. A larger screen is now ongoing.
“We now have an opportunity to find out why people get sick and do something about it,” says Harvard University’s Kevin Eggan PhD.
But experts caution that stem cell models alone may not be sufficient to discover new treatments for diseases – including ALS. “I think stem cells have huge potential to capture disease. But at the same time, its cells – not patients,” says Kyoto University’s and Gladstone Institutes’ Shinya Yamanaka MD PhD.
An emerging strategy is to use stem cell models to discover potential medicines for ALS. And, then validate them in emerging and existing mouse models of disease.
“I think it is very important to combine these technologies,” says Kyoto University’s Haruhisa Inoue MD PhD.
Stemming the ALS tide
ALS clinicians first turned to stem cells in the late 1990s in hopes to develop a treatment for the disease. More than 10 potential stem cell therapies are now being tested in ALS clinics worldwide.
The strategy aims to provide 'life support' to motor neurons in people with ALS or detoxify their nervous systems.
Stem cell transplantation into the spinal cord appears to be safe according to Neuralstem's phase I clinical trial results presented by Emory University neurosurgeon Nick Boulis MD at ISSCR13. Short-term side effects including dizziness and headache - expected due to nature of the surgical procedure according to Boulis. No acceleration of disease progression (ALS-FRS, FVC, HHD) was reported.
“We are not at the point of talking efficacy,” says Boulis.
A phase II clinical trial of Neuralstem’s NSI-266 neural stem cell (NSC) strategy is now enrolling. The study is expected to begin sometime later this year.
In the meantime, University of Michigan’s Simon Lunn PhD is working hard to develop Neuralstem 2.0. The treatment strategy, which uses re-engineered NSI-266 cells, aims to keep existing motor neurons healthy by delivering the neuroprotective substance IGF-1 directly to the diseased spinal cord. Preclinical testing in a superoxide dismutase 1 (SOD1) mouse model of ALS is ongoing.
Across the globe, in Israel, Brainstorm’s NurOwn is currently being tested at phase II. Six-month follow-up of 12 people with ALS treated with NurOwn either intramuscularly or intrathecally indicate that the drug appears to be safe according to phase I/II results presented at ISSCR13. No acceleration of disease progression (FVC, ALS-FRS) or adverse events were reported.
Astrocytes explode
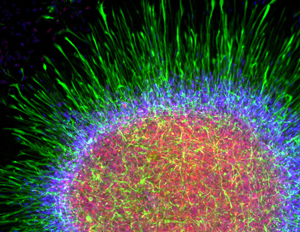
Clearing the CSF? Clinicians hope to detoxify the CNS in people with ALS by delivering glial restricted precursors (GRPs) which transform into astrocytes in the spinal cord. Image: Robert Krencik PhD, University of Wisconsin.
In the US, astrocyte replacement strategies are approaching the clinic. Spearheaded by Johns Hopkins University School of Medicine’s Nicholas Maragakis MD and University of California San Diego School of Medicine’s Larry Goldstein PhD and Martin Marsala MD, these potential treatments aim to protect motor neurons in people with ALS by introducing astrocytes to mop up excess glutamate that accumulates over the course of the disease. A phase I clinical trial is anticipated to be begin by 2014.
In Los Angeles, Cedar-Sinai’s Clive Svendsen PhD is taking a different approach – using human embryo-derived astrocytes to deliver potential ALS medicines directly into the spinal cord. The strategy aims to help keep existing motor neurons in people with ALS healthy by nourishing them with neuroprotective substances. The stem cell-based therapy, which involves the introduction of healthy GDNF-secreting astrocytes, is currently at the IND stage. A phase I clinical trial is anticipated to begin by 2014.
The art of anti-rejection
The immune system, however, remains a considerable barrier toward implementing these potential therapies in the clinic.
“The biggest source of problems is the immune system,” says Emory University’s Nick Boulis MD. Most people with ALS could not tolerate the anti-rejection drugs.
Currently, clinicians rely on broad immunosuppressive agents routinely recommended to people who receive organ transplants. But whether these medicines are the right choice for stem cell recipients remains an open question.
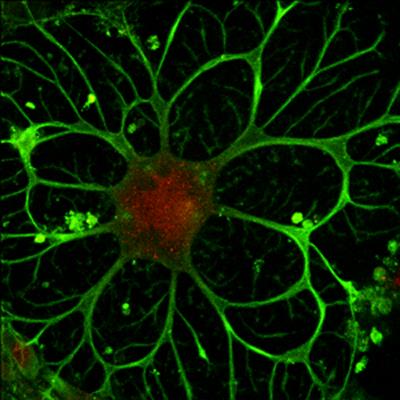
Immunoprivileged? Scientists remain unsure whether neural stem cells (above) trigger an immune response post-transplantation. Image: Yadong Huang MD PhD, Gladstone Institutes.
Clinicians simply do not know which if any of these potential treatments switches the immune system into attack mode – let alone which medicines might protect people from developing complications.
A growing number of researchers are turning to mouse models in hopes to answer these questions. Human embryo-derived treatment strategies were amongst the first to be evaluated.
“Embryonic stem cells have a level of immune-privilege – but eventually these cells are rejected,” explains Boston University School of Medicine’s Ashleigh Boyd PhD.
But the transplantation of cooked up neural precursors appears to be tolerated provided that these grafts are genetically identical according to recently published preclinical studies presented by Boyd at ISSCR 2013. No evidence of rejection was detected.
The results suggest that ‘autologous’ therapies, which involve re-engineering patients’ own stem cells, may evade immunosurveillance systems.
A growing number of stem cell experts however worry that these potential treatments may simply be too impractical to manufacture and therefore too difficult to implement into general clinical practice.
An emerging alternative is to create national immune system-typed stem cell banks which could be readily accessed – a strategy similar to that used in existing bone marrow and organ transplantation procedures. The approach according to a growing number of stem cell experts is simply more practical and cost-effective. Only 150 HLA-typed iPS lines are estimated to be needed to deliver care to most residents of the UK according to studies led by Cambridge University Teaching Hospitals’ Craig Taylor PhD FRCP.
An HLA-typed stem cell bank is already under construction in Japan. The project, led by Kyoto University’s Shinya Yamanaka MD PhD, is expected to be available to provide care to more than 90% of residents within the next ten years.
Anti-rejection medicines however are likely to be needed – at least for many of these potential stem cell treatments according to preclinical results presented by Nick Boulis MD.
“It is necessary to use some sort of immunosuppression,” says Boulis. “But we can probably use far less immunosuppressive drugs.”
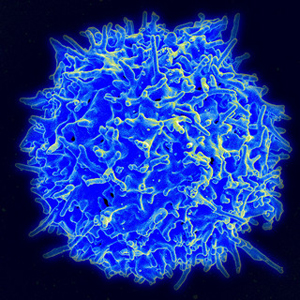
Short-term gains? Transient immunosuppression strategies, which reduce T-cell activation, may make stem cell treatment strategies more tolerable. Image: National Institute of Allergy and Infectious Diseases (NIAID).
But this is not because the neural stem cells themselves are being attacked according to preliminary preclinical studies presented by Nick Boulis MD.
The reason according to studies led by Stanford University School of Medicine cardiologist Joseph Wu MD PhD appears to be that anti-rejection medicines are needed to encourage the transplanted cells to settle in – engraft into the diseased tissues. But according to results presented at ISSCR 2013, these medicines might only be needed in the short-term.
iPS-based grafts appear to be detected at least one month post-tranplantation in the heart and muscles of mice treated for about a week with T cell co-stimulatory blockers CTLA4-Ig and anti-LFA1.
The emerging anti-rejection strategy targets the same mechanisms in people with ALS suspected to contribute to the progression of the disease.
Conventional immunosuppression medicines including cyclosporin A and sirolomus/tacrolimus however appear to be ineffective – at least in models of intramuscular transplants and heart disease.
The approach is growing acceptance in a number of disease indications – including ALS. In Los Angeles, Clive Svendsen PhD is developing transient immunosuppression strategies for people with ALS. Elsewhere in the US, Neuralstem clinicians are soon to begin implementing transient immunosuppression strategies – at least in the treatment of people with spinal cord injury. And, according to Neuralstem’s Karl Johe PhD, are considering using them in future clinical trials for ALS.
Technically speaking
An emerging stem cell beacon may soon facilitate the development of stem cell therapies for ALS. The tracker, called ferumoxytol, enables clinicians to track injected stem cells via MRI post-transplantation. The technique is expected to be especially helpful to inform dosing and numbers/sites of injection. Led by Emory University’s Nick Boulis MD, preclinical testing of Neuralstem’s NSI-266 neural stem cell therapy is ongoing.
A new tool may soon make the discovery of potential medicines for ALS even easier according to new results from MIT’s Feng Zhang PhD. An RNA-guided genome editing enzyme, called CRISPR, enables researchers to create human embryonic stem cells that differ specifically in a single genetic change at 58% efficiency. The resulting “isogenic” control lines ensure that the drugs discovered in stem cell models of ALS are likely relevant to the disease.
***
To learn more about stem cells and ALS, check out our interactive timeline Stem Cells Rolling Along in ALS. To learn more about discovering new medicines for ALS in cellular models of disease, check out iPS ready, set screen?