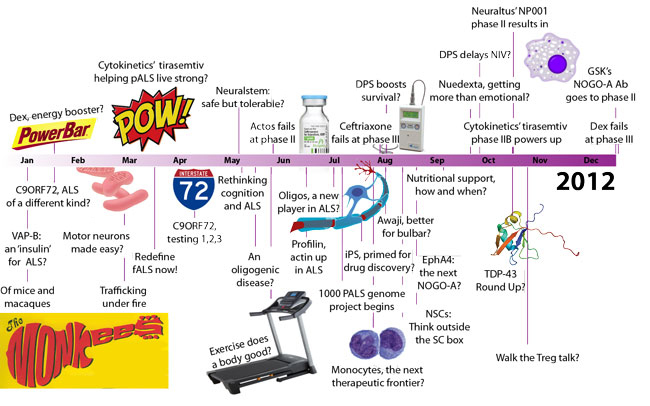
The year 2012 has now drawn to a close. ALS Today turns back the clock - highlighting key advances in 2012 and key challenges going forward.
Monocytes, T-cells and oligodendrocytes emerged as potentially key players that could be targeted in ALS. Advances in induced pluripotent stem (iPS) cell technologies opened the door toward the discovery of new medicines for the disease. Emerging antisense-based treatment strategies surfaced for C9- ALS, the most common form of ALS identified to date. GSK’s potential neuromuscular junction protector Ozanezumab (anti-NOGO A) approached phase II. And, Avanir’s emotionality-regulator Nuedexta, Novartis’ T cell sequesterer fingolimod (Gilenya), and the potential neuronal excitability-reducer mexiletine re-entered the pipeline – phase II clinical trials expected to begin sometime in 2013.
Key challenges, however, remain. The first clinical reports of C9-ALS reawakened the debate about how to define inherited forms of the disease (fALS) and test for them. Clinical trials launched in 2012 hope to establish evidence-based clinical practice guidelines for the NeuRX, NIV and feeding tube to help clinicians best meet their ALS patients’ respiratory and nutritional needs. And, the failure of ceftriaxone and dexpramipexole fueled the debate about which drugs to push forward in the clinic and how best to evaluate them.
Take a look back at 2012 by exploring our interactive timeline. Click on key advances and challenges ahead to learn more.
Images courtesy of Arcadian, Bradford Timeline, East Birmingham Hospital's Graham Beards MD, NIGMS' Judith Stoffer.